Dental case acceptance is the percentage of recommended treatment plans that patients agree to and schedule. Most practices aim for 85% or higher on single-visit treatments and 50 to 65% on larger, multi-visit plans. The national average sits closer to 50 to 60% overall, which means a significant portion of diagnosed dentistry never gets done.
That gap is not just a revenue problem. It is a care problem. When patients decline treatment they need, conditions progress, costs rise, and outcomes suffer. Improving case acceptance means more patients getting healthier, not just more production coming through the door.
According to Dental Economics, the breakdown rarely happens at the clinical level. Most dentists are diagnosing correctly. The breakdown happens in how the need is explained, how value is framed, and how the patient feels during the decision-making moment. That is where most practices have the most room to improve.
Why Patients Say No to Recommended Treatment
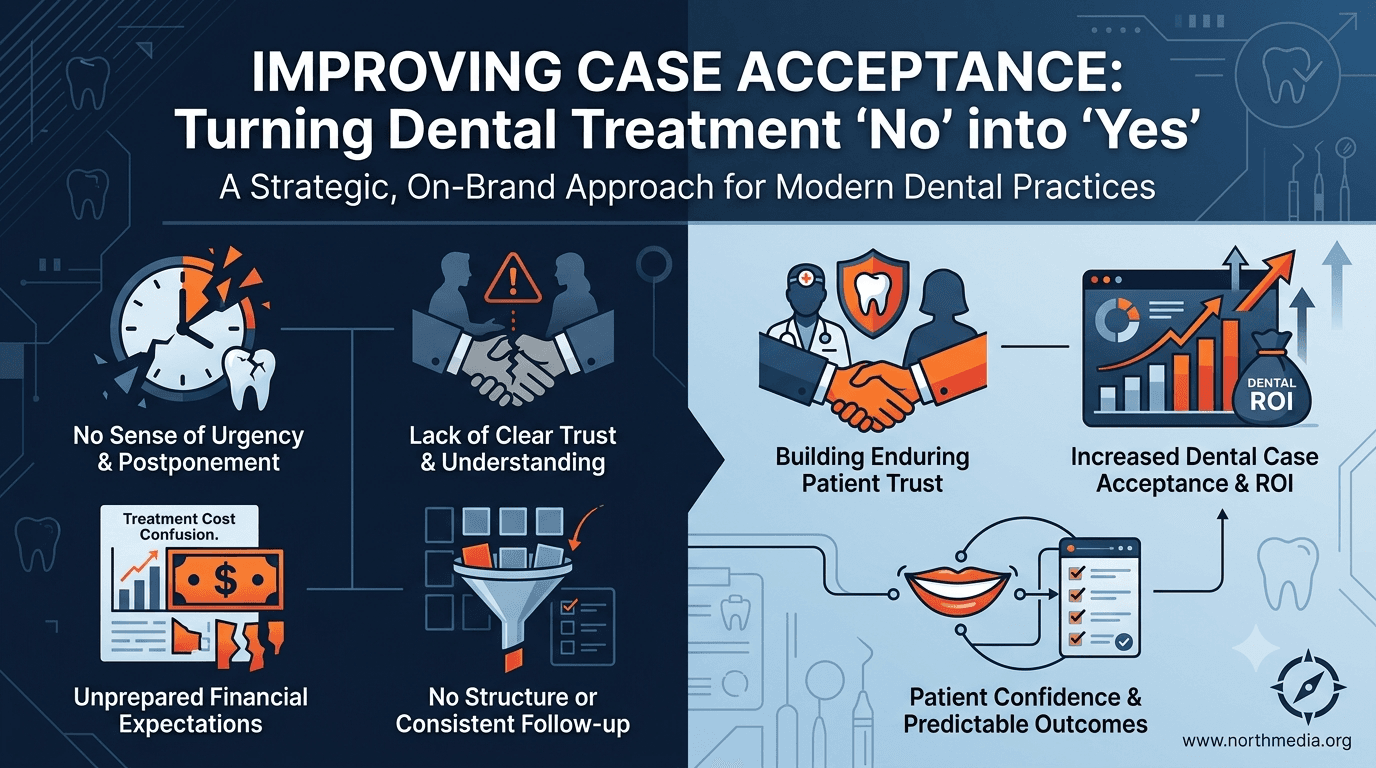
Before you can improve your numbers, you need to understand what is actually driving the decline.
1. The patient does not feel the urgency. When treatment feels optional, patients delay. Clinical language often fails to communicate consequence. A patient hears "you have a crack" but not what happens if they ignore it for six months.
2. The patient does not trust the recommendation. Trust is built long before the treatment plan is presented. Patients who feel rushed, unheard, or like they are being upsold are far more likely to decline. First-visit case presentations carry the highest risk.
3. The cost came as a surprise. Presenting a large fee without context, without financing options, or without a clear sense of value creates hesitation. Most patients are not unwilling to pay. They are unwilling to pay for something they do not fully understand or believe in yet.
4. The patient needed time but had no structure. Some patients genuinely need to think. Practices without a follow-up process lose these cases by default. No follow-up is a passive no.
5. The conversation was clinical, not personal. When the discussion centers on procedures, codes, and findings rather than what the patient actually cares about, the emotional connection fails. Patients accept treatment when they can connect it to their daily life, their comfort, and their confidence.

How Communication Style Directly Affects Case Acceptance
Paul Homoly, one of the most respected voices in dental case acceptance, built his entire framework around a simple idea: patients do not buy dentistry, they buy relationships. His work makes a consistent case that clinical excellence alone does not produce high acceptance rates. Dentists who communicate as trusted advisors, rather than technical experts delivering a verdict, consistently outperform their peers.
The most effective shift is moving from a presentation to a conversation. Instead of walking a patient through a treatment plan using procedure names and clinical findings, you walk them through their own situation in plain language. What is happening. What it means for their daily life. What their options are.
The dentist who leads with empathy before evidence will always have an easier time earning a yes. Patients need to feel like they are being guided, not sold to.
Key communication principles that move the needle:
Use the patient's own words to reflect their symptoms or concerns back to them
Explain consequences in lifestyle terms, not clinical ones
Ask permission before presenting: "Can I walk you through what I found and what I'd recommend?"
Pause after presenting and allow silence; do not immediately justify or discount
Respond to hesitation with curiosity, not defensiveness
These are learnable skills, and they are coachable skills for treatment coordinators and front-desk staff as well.
The Role of the Treatment Coordinator in Case Acceptance
In higher-performing practices, the dentist diagnoses and introduces the treatment, then hands off to a trained treatment coordinator for the financial and scheduling conversation. This separation works because it removes the awkwardness of a clinician discussing fees and lets each role stay in its lane.
A treatment coordinator's job is not to close a sale. It is to remove barriers and help the patient feel confident moving forward. Patients sense the difference immediately, and it changes how they respond.
What an effective treatment coordinator does:
Restates the clinical findings in plain terms to confirm understanding
Walks through the financial breakdown clearly, including insurance estimates and out-of-pocket costs
Introduces financing options as a standard part of the conversation, not a last resort
Addresses hesitation by asking questions rather than adding pressure
Sets a follow-up call before any patient leaves undecided
Practices without a dedicated treatment coordinator often see the doctor or front desk absorbing this role inconsistently. That inconsistency is one of the most common hidden causes of lower-than-expected case acceptance.
Structuring the Treatment Presentation for Better Results
The format of how treatment is presented matters as much as the content. A rushed, disorganized, or impersonal presentation leaves patients with too many unresolved questions to feel comfortable saying yes.
A reliable structure looks like this:
Step 1: Acknowledge what the patient came in for. Ground the conversation in something they care about before moving into clinical findings.
Step 2: Share findings in plain language. Use images, X-rays, or intraoral camera footage wherever possible. Visual evidence increases acceptance significantly because patients can see the problem rather than just being told about it.
Step 3: Explain the consequence of not treating. This step gets skipped most often. Patients need to understand what progresses, what becomes more costly, and what quality-of-life impact they face if they wait. Keep it honest and factual, not alarming.
Step 4: Present options, leading with your recommendation. Offering options gives patients a sense of control without undermining clinical guidance. Lead with what you believe is best for them, and explain why.
Step 5: Invite questions before moving to financials. Give the patient space to respond to the clinical conversation before cost enters the picture. Mixing the two creates confusion.
Step 6: Walk through the financial details clearly. Cover total cost, insurance estimate, and available financing. Where appropriate, frame monthly payment options in terms of weekly or daily cost to make them more tangible.
Step 7: Ask for the next step, not the yes. Instead of asking whether they want to proceed, ask which scheduling option works better for them. A small forward-motion question is far easier to agree to than a large commitment question.
How to Address Financial Barriers Without Discounting
Cost is real. But defaulting to discounts as a response to hesitation undermines both profitability and perceived value. The goal is to make the investment feel manageable and worth it, not cheaper.
Introduce third-party financing proactively. Financing options should be part of the standard conversation, not pulled out only when a patient says they cannot afford it. Framing it as "most patients choose one of these two options" normalizes the approach and removes stigma.
Break large treatment plans into phases. For significant or comprehensive treatment, phasing work over multiple appointments or payment periods reduces the perceived financial barrier without reducing what gets done. Present the full plan first, then offer a phased approach as a practical path forward.